")
If you’re thinking about ICL surgery while going through chemotherapy, you need to slow the decision down and look at the bigger clinical picture first. On paper, Implantable Collamer Lens procedures are predictable and highly effective, but chemotherapy changes how your body behaves at a cellular level. You’re not dealing with a standard elective case anymore you’re working with suppressed immunity, altered healing, and variable systemic stability.
One of the biggest mistakes patients make is assuming eye surgery is “local” and therefore unaffected by systemic treatment. It isn’t. Chemotherapy can reduce white blood cell counts, increase infection risk, and delay tissue repair, all of which directly impact surgical safety and recovery. Even if the eye itself appears healthy, your body’s ability to respond to surgical trauma is not operating at full capacity.
You also need to consider how chemotherapy affects the ocular surface and internal eye environment. Dry eye, inflammation, and fluctuating vision are common during treatment, and these can interfere with both pre-operative measurements and post-operative outcomes. If your baseline isn’t stable, your surgical planning won’t be either and that introduces avoidable risk into what should be a highly controlled procedure.
What Is ICL Surgery and How Does It Work?
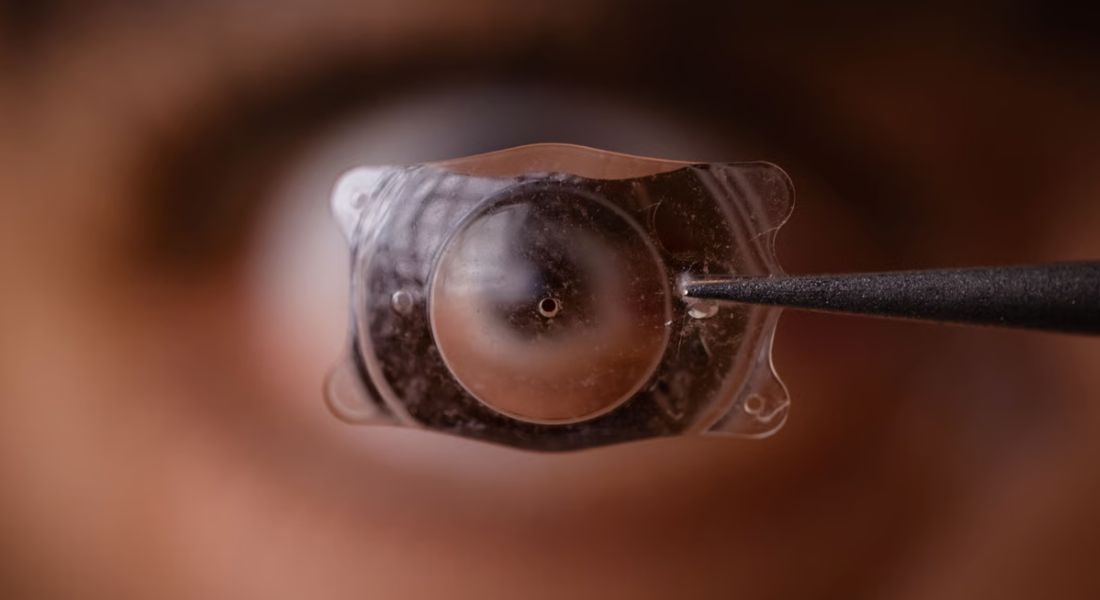
ICL surgery is a refractive procedure where a soft, biocompatible lens is implanted inside your eye to correct vision with high precision. The lens sits behind your iris and in front of your natural lens, working with your eye’s existing optics rather than reshaping them. This means you’re achieving correction without altering the cornea, which is a key distinction from laser-based procedures.
What makes this approach clinically attractive is that it’s both additive and reversible. You’re not removing tissue you’re inserting a lens that can be adjusted or removed if needed, which gives you more flexibility over the long term. It’s particularly useful if your corneal thickness or prescription makes laser correction less predictable, and the procedure itself is typically efficient, done under local anaesthetic with minimal intraoperative discomfort.
Where you need to be careful is in assuming recovery will follow the standard pathway if you’re undergoing chemotherapy. In a healthy system, healing is usually straightforward and predictable, but chemotherapy changes that equation. Your recovery timeline, infection risk, and inflammatory response can all shift, which is why surgical timing and proper medical clearance aren’t optional they’re critical to getting a safe and stable outcome.
How Chemotherapy Affects the Body
Chemotherapy doesn’t just target cancer it disrupts every fast-moving system your body relies on to recover from stress, including surgery. You’re dealing with a treatment that actively suppresses cell turnover, which means healing, repair, and immune defence are all operating below normal capacity. That shift is manageable in oncology, but it becomes a constraint when you introduce elective procedures like ICL.
The most immediate concern is immune suppression. Your white blood cell count can drop to levels where even minor surgical exposure increases infection risk, and your body’s response to that infection is slower and less effective. What would normally be a low-risk, controlled procedure now carries a different profile because your baseline defence system isn’t fully functional.
You also need to factor in how chemotherapy affects blood parameters and tissue integrity. Reduced platelet counts can influence bleeding risk, while impaired cellular repair slows down recovery at the microscopic level. Add to that an increased inflammatory response, and you’re looking at a healing process that is less predictable, more reactive, and harder to manage exactly the scenario you want to avoid when planning precision eye surgery.
Effects of Chemotherapy on Eye Health
Chemotherapy doesn’t leave the eyes untouched, and you’ll often see the impact show up in ways that directly interfere with surgical planning. Dryness, irritation, and unstable tear film are some of the most common issues, and they’re not just minor discomforts they affect how accurately your vision can be measured. If your ocular surface isn’t stable, your pre-operative calculations for ICL power can be off, which compromises the final result.
You also need to consider deeper effects beyond the surface. Chemotherapy can trigger inflammation, increase light sensitivity, and cause fluctuations in vision that come and go throughout treatment cycles. These variations make it difficult to establish a reliable baseline, and without that, you’re effectively planning surgery on shifting ground. That’s not a position you want to be in when precision is critical.
Before you even think about proceeding, your eye health needs to be stable and predictable. Any dryness, inflammation, or surface irregularity should be treated and resolved first, not managed alongside surgery. A thorough assessment isn’t just a formality it’s how you confirm that your eyes can handle the procedure and deliver a consistent, safe outcome.
Why Timing Matters for ICL Surgery
When you’re considering ICL surgery after chemotherapy, timing isn’t just a detail it directly affects your safety and results. You might feel ready to move forward quickly, but your body needs time to recover from the impact of treatment. If surgery is done too early, the risks increase, and the outcome may not meet expectations.
- Immune System Recovery Is Non-Negotiable: Chemotherapy can significantly suppress your immune system, making you more vulnerable to infections. If you undergo surgery during this phase, even minor complications can escalate, so waiting until your immune response stabilises is essential for safe healing.
- Blood Counts Need to Normalise: Your white blood cells, platelets, and haemoglobin levels all play a role in recovery. Low counts can increase bleeding risk, slow healing, and reduce your body’s ability to fight infection, which is why surgeons rely on stable lab results before proceeding.
- Healing Capacity Must Be Restored: After chemotherapy, your body’s natural repair mechanisms are often compromised. Rushing into surgery can lead to delayed healing or unpredictable results, so giving your tissues time to regain normal function improves both safety and visual outcomes.
- Overall Health Should Be Stable: It’s not just about one parameter; your entire system needs to be back to baseline. Energy levels, nutrition, and organ function all influence how well you tolerate and recover from surgery, making a full health assessment critical.
- Specialist Coordination Reduces Risk: Your oncologist and eye specialist will evaluate your readiness together rather than in isolation. This collaborative approach ensures that your cancer recovery isn’t disrupted while also confirming that your eyes are in the best possible condition for surgery.
Taking a measured approach with timing gives you the best chance of a smooth procedure and strong visual results. When you allow your body to fully recover and rely on coordinated medical advice, you reduce unnecessary risks and set yourself up for a safer, more predictable outcome.
Immune Suppression and Surgical Risk
When your immune system is suppressed, even a well-controlled procedure like ICL surgery carries a different level of risk. You’re still entering the eye, and that creates a pathway however small for infection. Under normal conditions, your body and standard sterile protocols manage this effectively, but during chemotherapy, your ability to respond is reduced, and that changes the equation.
The concern isn’t just the chance of infection, but how your body handles it if it occurs. Intraocular infections, while rare, can escalate quickly and require aggressive treatment. If your immune response is compromised, the early warning signs may be muted and the progression more difficult to control, which is why surgeons take a far more cautious stance in this phase.
This is exactly why timing becomes a clinical decision, not a personal preference. Delaying surgery until your immune markers recover particularly white blood cell counts brings the risk profile back to a safer baseline. It’s not about postponing unnecessarily; it’s about ensuring that when you do proceed, your body is in a position to protect you and support a stable recovery.
Healing and Recovery Considerations
Healing after ICL surgery is usually predictable, but chemotherapy disrupts that predictability in ways you can’t afford to ignore. You’re relying on precise tissue recovery inside the eye, and when cellular repair is slowed, everything from wound sealing to visual stabilisation takes longer. That delay isn’t just inconvenient it increases exposure to secondary issues like irritation, fluctuating vision, and prolonged dependence on medication.
You’ll also see a different inflammatory profile. Instead of a short, controlled response, inflammation can become more persistent and harder to settle, which directly affects comfort and visual clarity. This means your post-operative plan often needs to be more intensive longer courses of anti-inflammatory drops, closer follow-up intervals, and tighter control of any emerging symptoms.
The practical takeaway is simple: outcomes improve when your body is ready. Once chemotherapy effects have stabilised and your recovery systems are functioning properly, healing becomes faster, cleaner, and far more predictable. Waiting isn’t a setback it’s how you protect the result and avoid turning a straightforward procedure into a prolonged recovery process.
When Is It Safe to Consider ICL Surgery?
You don’t approach ICL surgery with a fixed timeline after chemotherapy you approach it with clinical evidence that your body is ready. The baseline requirement is systemic stability, which means your blood work, immune function, and overall recovery have returned to acceptable levels. Until that point, you’re not planning surgery you’re still in recovery mode.
The first gate is medical clearance. Your oncologist needs to confirm that your white blood cell count, platelets, and general health profile can support a surgical procedure without elevated risk. Without that sign-off, moving forward isn’t just premature it’s unsafe. Even if you feel fine subjectively, decisions here are driven by measurable data, not perception.
Once you’re medically cleared, the focus shifts to ocular readiness. Your eye surface must be stable, your measurements consistent, and there should be no residual inflammation or chemotherapy-related changes affecting vision. This is where a detailed pre-operative assessment becomes critical, because you’re confirming that both your body and your eyes are aligned for a predictable outcome.
The Role of Medical Clearance
Medical clearance isn’t a formality it’s a hard clinical checkpoint that determines whether you proceed or not. Your oncology team is the only group with full visibility on how your body has responded to chemotherapy, including immune recovery, blood counts, and any lingering systemic effects. Without that input, you’re making a surgical decision with incomplete data, and that’s where risk creeps in.
From a surgical planning perspective, your eye specialist relies on this clearance to define timing, not just approval. We’re looking at parameters like neutrophil count, platelet levels, and overall systemic stability to assess whether your body can tolerate both the procedure and the recovery phase. If those markers aren’t within a safe range, the plan shifts either delayed or re-evaluated because forcing the timeline never ends well.
The real value comes from coordination. When your oncologist and eye surgeon are aligned, decisions become precise rather than cautious guesses. That multidisciplinary approach reduces complications, tightens recovery expectations, and ensures you’re not overlooking hidden risks. Even if you feel completely fine, you don’t bypass this step because what matters here isn’t how you feel, it’s how your body is actually performing under the surface.
Potential Risks if Surgery Is Done Too Early
It’s completely understandable to want to move ahead with ICL surgery as soon as possible, especially once chemotherapy is behind you. But if you act too early, your body may not be ready to handle the stress of surgery. This is where complications start to creep in, and what should be a straightforward procedure can become unnecessarily complex.
- Higher Risk of Infection: When your immune system hasn’t fully recovered, your body is less equipped to fight off bacteria. Even with sterile surgical conditions, the risk increases, and infections in the eye can be serious, sometimes requiring intensive treatment or delaying recovery significantly.
- Delayed Healing Response: Your body’s ability to repair tissue is often compromised after chemotherapy. This means surgical sites may take longer to heal, increasing discomfort and extending your recovery timeline beyond what’s typically expected.
- Increased Inflammation: An unstable immune response can trigger excessive inflammation after surgery. This not only affects comfort but can also interfere with visual clarity and require additional medication or monitoring to control.
- Unpredictable Visual Outcomes: If your eyes and overall health aren’t stable, your results may not be consistent. Vision may fluctuate or take longer to settle, which can be frustrating and may even require further corrective steps.
- More Frequent Follow-Ups and Interventions: Early complications often mean more appointments, more treatments, and more stress. What could have been a smooth, single recovery phase may turn into an extended process with added medical oversight.
Taking a step back and allowing your body to fully recover puts you in a much stronger position for surgery. When you prioritise timing over urgency, you reduce complications and give yourself the best chance of a smooth recovery and stable, long-term visual results.
Managing Dry Eye and Ocular Surface Health

Dry eye is one of the most underestimated variables in ICL planning, especially after chemotherapy. You’re not just dealing with discomfort you’re dealing with an unstable ocular surface that directly affects measurement accuracy and post-operative recovery. If the tear film is inconsistent, your biometry and lens calculations can be off, and that’s how you end up compromising an otherwise precise procedure.
You need to treat the surface first, not alongside surgery. That means structured lubrication, not occasional drops, combined with targeted interventions if required anti-inflammatory therapy, tear film stabilisation, and in some cases lid margin management. The goal is to normalise the ocular environment so your measurements are repeatable and your healing response is controlled from day one.
From a workflow perspective, you don’t move forward until the surface proves it’s stable. That means consistent readings across visits, reduced symptoms, and no active inflammation. Once that baseline is locked in, your surgical plan becomes far more reliable, and your recovery follows a cleaner, more predictable path. Preparation here isn’t optional it’s what protects your outcome.
Emotional Considerations for Patients
Balancing recovery from chemotherapy with the desire to move forward especially with something like vision correction can feel mentally draining. You’re trying to regain control and normality, and clear vision often becomes part of that goal. But if you push the timeline ahead of your body’s readiness, you risk turning a positive step into a setback, and that’s not a trade-off worth making.
What you’re feeling impatience, uncertainty, even frustration is completely expected in this phase. The key is to replace guesswork with clarity. When your oncologist and eye specialist communicate clearly with you, the process becomes structured rather than overwhelming, and you start making decisions based on evidence instead of emotion.
A staged approach works best in practice. You stabilise your systemic health first, then your ocular surface, and only then move towards surgery. That sequence protects your outcome and reduces stress because each step is validated before the next begins. When you follow that order, you’re not delaying progress you’re ensuring that when you do proceed, everything is working in your favour.
Long-Term Outcomes After Chemotherapy
Once you’ve fully recovered from chemotherapy, ICL surgery behaves exactly as it should predictable, stable, and highly effective. At that point, you’re no longer dealing with compromised healing or immune suppression, so the procedure returns to its standard risk profile. From a surgical standpoint, outcomes are driven by precision and planning, not by your past treatment history.
There’s no clinical evidence suggesting that previous chemotherapy reduces the effectiveness of ICL once your body has normalised. What matters is your condition at the time of surgery, not what you’ve gone through before. If your ocular surface is stable, your measurements are consistent, and your systemic health is cleared, you can expect the same level of visual improvement and long-term stability as any other suitable candidate.
Where you need to stay disciplined is in follow-up and long-term monitoring. Regular eye examinations ensure that lens positioning, intraocular pressure, and overall eye health remain optimal over time. When the procedure is timed correctly and supported by proper aftercare, satisfaction rates are high and outcomes remain consistent this is where planning pays off, turning a delayed decision into a well-executed one.
Importance of Specialist Consultation

Specialist consultation is where this entire decision either becomes precise or stays risky. You’re not dealing with a routine refractive case post-chemotherapy patients require layered evaluation, and that only comes with experience. A seasoned eye specialist doesn’t just check eligibility; they assess timing, systemic recovery, ocular stability, and how all of that interacts with surgical planning.
In practice, a proper consultation goes beyond standard testing. You’re looking at repeatable measurements, detailed anterior chamber analysis, tear film stability, and a full review of your medical history alongside oncology input. The key here is coordination your eye surgeon and oncologist need to be aligned so decisions are based on real data, not assumptions. That’s how you reduce variability and keep the procedure controlled.
Relying on generic timelines is where most mistakes happen. Your recovery curve, immune status, and ocular condition are unique, and your surgical plan should reflect that. When you work with the right specialist, you’re not guessing when it’s safe you’re confirming it step by step, which is exactly how you protect both your vision and your overall health.Top of Form
FAQs:
1. Can I have ICL surgery while undergoing chemotherapy?
No, this is generally not recommended. Chemotherapy suppresses your immune system and affects healing, which increases the risk of infection and complications during and after surgery.
2. How long should I wait after chemotherapy before considering ICL surgery?
There’s no fixed timeline. You should wait until your oncologist confirms that your immune system, blood counts, and overall health have returned to stable levels.
3. Why is immune recovery important before ICL surgery?
Your immune system plays a key role in preventing infection and supporting healing. If it’s compromised, even minor surgical procedures can carry higher risks and slower recovery.
4. Does chemotherapy affect eye health directly?
Yes, it can cause dry eye, irritation, inflammation, and fluctuating vision. These issues can interfere with both surgical planning and post-operative outcomes.
5. Can dry eye delay ICL surgery?
Absolutely. An unstable tear film affects measurement accuracy and healing. Your ocular surface needs to be stabilised before surgery to ensure reliable results.
6. Is ICL surgery safe after full recovery from chemotherapy?
Yes, once your body has fully recovered and you have medical clearance, ICL surgery typically returns to its normal safety and success profile.
7. What role does my oncologist play in the decision?
Your oncologist provides essential medical clearance by confirming your immune status, blood counts, and overall readiness for surgery. This step is non-negotiable.
8. What happens if I have ICL surgery too early after chemotherapy?
You increase the risk of infection, delayed healing, excessive inflammation, and unpredictable visual outcomes. This can turn a routine procedure into a prolonged recovery.
9. Will chemotherapy affect the long-term results of ICL surgery?
Not if you wait until full recovery. Once your body stabilises, outcomes are comparable to those of patients who have not undergone chemotherapy.
10. How do specialists decide if I’m ready for ICL surgery?
They assess a combination of factors including blood work, immune recovery, ocular surface stability, and consistent eye measurements, often in coordination with your oncology team.
Final Thought: Prioritising Safety for the Best Outcome
When you’re considering vision correction after chemotherapy, the most important decision isn’t if you can have ICL surgery, but when you should have it. Your body needs to be fully recovered, your immune system stable, and your eyes in a predictable, healthy state before moving forward. Taking a patient, medically guided approach ensures that the procedure remains as safe, precise, and effective as it’s designed to be. Rushing this process can introduce avoidable risks, while proper timing allows you to benefit from the full potential of the treatment. If you’re considering ICL surgery in London, you can get in touch with us at London Cataract Centre.
References:
1. Jabbour, S. and Bower, K.S. (2021) Three-year outcomes of implantable collamer lens followed by excimer laser enhancement (“Bioptics”), Clinical Ophthalmology, 15, pp. 635–643. Available at: https://pmc.ncbi.nlm.nih.gov/articles/PMC7896759/
2. Omoti, A.E. and Omoti, C.E. (2006) Ocular toxicity of systemic anticancer chemotherapy, Pharmacy Practice, 4(2), pp. 55–59. Available at: https://pubmed.ncbi.nlm.nih.gov/25247000/
3. Packer, M. (2018) The Implantable Collamer Lens with a central port: review of the literature, Clinical Ophthalmology, 12, pp. 2427–2438. Available at: https://pmc.ncbi.nlm.nih.gov/articles/PMC6267497/
4. Zemba, M., et al. (2021) Ocular side effects of cancer therapy: A comprehensive review, Journal of Clinical Medicine, 10(21), 5059. Available at: https://www.mdpi.com/2072-6694/16/2/344
5. Kapoor, G., et al. (2025) Objective and subjective outcomes following implantable collamer lens (ICL) implantation for the correction of myopia, Oman Journal of Ophthalmology. https://pubmed.ncbi.nlm.nih.gov/40666761/