")

If you’re reading this, there’s a good chance you’ve reached that frustrating stage of life where your arms suddenly feel too short. Menus blur. Phone screens need more light. Reading glasses appear in every room, yet are never where you left them. Presbyopia has arrived, whether you invited it or not.
At some point, many people start wondering if there’s a way off the constant glasses carousel. Laser eye surgery might sound tempting, but you may already have been told it won’t truly fix the problem. That’s usually when refractive lens exchange enters the conversation.
I want to take you through this properly, without hype or shortcuts. I’ll explain how refractive lens exchange works for presbyopia, whether the results really are permanent, and what kind of spectacle independence you can realistically expect over the long term. My goal is simple: help you decide whether this procedure makes sense for you.
Understanding presbyopia in plain terms
Presbyopia isn’t a disease or a problem with your eyes. It’s a natural part of ageing that affects everyone over time. Inside the eye is the crystalline lens, which allows you to focus smoothly at different distances when you’re young.
As you get older, this lens gradually stiffens and becomes less flexible. This makes focusing on near objects harder, usually starting in the early to mid-40s. Small print, phone screens, and low light become more challenging than before.
Over time, near vision continues to decline even if distance vision stays clear. Most people eventually need reading glasses or another form of correction. Presbyopia can’t be prevented, but it can be managed effectively once you understand what’s happening.
Why glasses and contact lenses only manage symptoms
Presbyopia isn’t a disease or a fault in your eyes. It’s a natural part of ageing that affects everyone over time. Inside the eye sits the crystalline lens, which allows you to focus smoothly at different distances when you’re young.
As you get older, this lens gradually stiffens and becomes less flexible. This makes focusing on near objects harder, usually beginning in the early to mid-40s. Small print, phone screens, and reading in low light often become more challenging.
Over time, near vision continues to decline even if distance vision remains clear. Most people eventually need reading glasses or another form of correction. Presbyopia can’t be prevented, but it can be managed effectively once you understand what’s happening.
Why laser eye surgery doesn’t truly solve presbyopia
Presbyopia isn’t a disease or a fault in your eyes. It’s a natural part of ageing that affects everyone over time. Inside the eye sits the crystalline lens, which allows you to focus smoothly at different distances when you’re young.
As you get older, this lens gradually stiffens and becomes less flexible. This makes focusing on near objects harder, usually beginning in the early to mid-40s. Small print, phone screens, and reading in low light often become more challenging.
Over time, near vision continues to decline even if distance vision remains clear. Most people eventually need reading glasses or another form of correction. Presbyopia can’t be prevented, but it can be managed effectively once you understand what’s happening.
What refractive lens exchange does differently
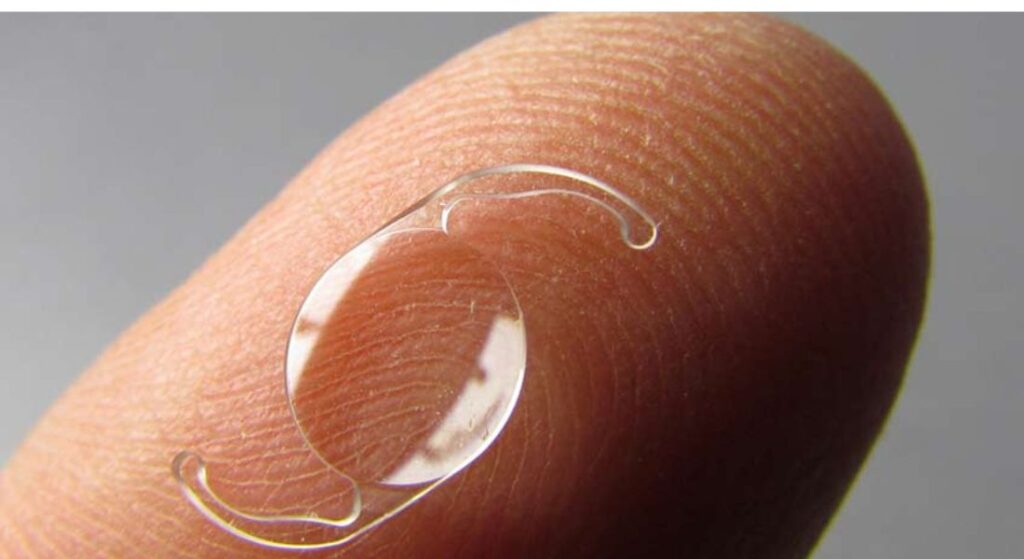
Refractive lens exchange, or RLE, takes a completely different approach to vision correction. Instead of reshaping the cornea, the eye’s natural lens is removed and replaced with an artificial intraocular lens. In practical terms, it is cataract surgery performed earlier, before a cataract has developed.
- Lens replacement rather than corneal reshaping: RLE corrects vision by changing the eye’s natural lens, which is responsible for focusing light. This avoids the limitations associated with altering corneal shape.
- Direct treatment of presbyopia: By replacing the ageing lens, RLE removes the underlying cause of presbyopia rather than compensating for it. This allows for more complete and stable vision correction.
- Stable, long-term optical results: Because the artificial lens does not age or lose flexibility, vision remains consistent over time. Results are not dependent on corneal healing or long-term biomechanical stability.
- Independence from corneal variables: Unlike laser procedures, outcomes are not affected by corneal thickness or structural changes. This makes results more predictable for a wider range of patients.
Refractive lens exchange offers a fundamentally stable form of vision correction by replacing the eye’s natural lens. This is why many people view RLE as a long-term solution rather than a temporary fix. Naturally,
How refractive lens exchange corrects presbyopia
Once the natural lens is removed, it can no longer stiffen or lose flexibility over time. The artificial lens implanted during refractive lens exchange does not age in the same way and remains optically stable for life.
Presbyopia is corrected not by forcing the eye to focus, but by replacing the lens responsible for the problem. Depending on the type of intraocular lens chosen, vision can be restored across near, intermediate, and distance ranges.
This range of focus is created through advanced lens design rather than muscular accommodation. The result is functional near vision without relying on the eye’s natural focusing mechanism.
What “permanent” really means in eye surgery
It’s important to be precise with language. When surgeons describe refractive lens exchange as permanent, they mean the correction itself does not regress. The artificial lens does not lose power, and presbyopia does not return.
That said, permanent does not mean your eyes will never change in any way. Other age-related eye conditions can still develop over time, such as macular degeneration or glaucoma.
Refractive lens exchange permanently removes presbyopia caused by lens ageing. It does not freeze your eyes in time, but it does eliminate one major cause of visual decline for good.
Why presbyopia cannot come back after RLE
Presbyopia is caused by the gradual stiffening of the eye’s natural lens. Once that lens is removed, the mechanism responsible for presbyopia is gone. There is simply nothing left to stiffen over time.
This is what makes refractive lens exchange fundamentally different from laser eye surgery. Laser reshapes the cornea but leaves the ageing lens in place, so presbyopia continues to progress. RLE removes the source of the problem entirely. From a presbyopia perspective, the result is genuinely permanent.
The role of intraocular lens choice
This is the stage where your expectations really need careful management. Not all intraocular lenses work in the same way, and each one creates a different visual experience. Understanding these differences helps you avoid surprises later.
Monofocal lenses give very clear vision at one set distance, usually far. Multifocal and extended depth-of-focus lenses spread vision across near, intermediate, and distance ranges. This can reduce your need for glasses, but it may involve compromises such as glare or reduced contrast.
Every option comes with trade-offs. Some lenses prioritise sharpness, while others focus on convenience and spectacle independence. Choosing the right lens is just as important as the surgery itself, because it shapes how you use your vision every day.
Spectacle independence: what’s realistic long term?
This is one of the most important conversations to have before surgery. Many people hope refractive lens exchange will mean never wearing glasses again. For some, that’s very close to reality, while others may still need them occasionally.
Advanced lens designs can provide a high degree of independence. Most patients can read, use screens, and drive without glasses. Everyday life becomes much easier, with less reliance on corrective lenses.
That said, very fine print in low light or prolonged close work may still benefit from minimal optical help. Absolute freedom from glasses is possible, but not guaranteed. Setting realistic expectations usually leads to the greatest satisfaction.
Adaptation and the brain’s role
Your brain plays a crucial role in how successful refractive lens exchange (RLE) feels. With multifocal or extended-range lenses, the brain gradually learns to prioritise the correct focal point depending on the task. This neural adaptation is an essential part of achieving optimal vision.
- Neural adjustment to new lenses: After RLE, the brain needs time to interpret visual information from multifocal or extended-range lenses. It learns to switch focus automatically between near, intermediate, and distance vision.
- Temporary visual fluctuations: During the adaptation period, which can last weeks or even months, vision may fluctuate slightly. Some patients experience mild halos or glare, particularly in low-light conditions, which is normal.
- Gradual improvement over time: Most patients find these temporary effects reduce as the brain adjusts. Vision becomes clear, comfortable, and reliable across multiple distances.
- Importance of patience: Allowing time for neural adaptation is key to achieving the full benefit of RLE. Understanding this process helps manage expectations and ensures satisfaction with the outcome.
The brain’s role in adapting to new lenses is central to the success of refractive lens exchange. Temporary visual disturbances are normal and usually improve over weeks or months. Patience during this adjustment period ultimately leads to clear, comfortable vision at all distances.
Why age matters when considering RLE for presbyopia
Refractive lens exchange is generally not recommended for younger patients with minimal presbyopia. If your natural lens still has significant flexibility, removing it may not be the best choice.
Once presbyopia is established, the balance changes. Many people start considering RLE in their late 40s, 50s, or early 60s, when the natural lens is already limiting near vision.
At this stage, the procedure often feels less like a sacrifice and more like an upgrade. It can restore functional vision and reduce dependence on reading glasses, making daily life noticeably easier.
RLE versus waiting for cataracts
Some people wonder whether it’s better to wait until cataracts develop naturally. Cataracts are a clouding of the lens that usually occurs later in life, while refractive lens exchange preempts this process.
Choosing RLE earlier gives you improved vision immediately, rather than waiting years for cataracts to affect sight. It also avoids the gradual visual decline that often precedes cataract surgery.
For many patients, the decision is less about medical necessity and more about quality of life. RLE offers clear, stable vision sooner, which can make daily activities easier and more enjoyable.
Safety considerations for presbyopia patients
Refractive lens exchange is an intraocular procedure, so it carries different risks compared with laser eye surgery. However, it is based on cataract surgery, one of the most frequently performed operations worldwide, and its safety profile is well understood.
For presbyopic patients, especially those with higher prescriptions, the risk-benefit balance often favours RLE over corneal laser procedures. The long-term stability and predictability of the artificial lens make it a reliable option.
Choosing an experienced surgeon and a specialist centre is critical. Expertise, careful planning, and the right facility significantly reduce risks and improve outcomes.
Night vision, glare, and halos
This topic deserves honesty. Some lens designs can cause visual phenomena, such as halos or glare, especially at night. These effects are usually more noticeable early on and often diminish as your brain adapts.
Not every patient experiences them, and severity can vary widely for those who do. Understanding your own sensitivity is important.
A thorough consultation should explore your lifestyle and tolerance for these effects, helping to match the lens choice to your daily needs.
Driving, screens, and modern visual demands

Modern life places heavy demands on our eyes. Driving at night, working on computers, using smartphones, and reading tablets all require frequent changes in focus. Presbyopia makes this juggling act harder, leading to eye strain, fatigue, and frustration.
Refractive lens exchange can simplify daily life by reducing the need to switch between different pairs of glasses constantly. Many patients report a sense of visual ease and comfort they haven’t experienced in years.
This functional improvement often outweighs minor compromises, allowing clearer vision across multiple tasks. Everyday activities feel more natural, whether at work, on the road, or enjoying leisure time.
Longevity of visual outcomes
Once implanted, intraocular lenses do not wear out and are made from highly biocompatible materials designed to last a lifetime. They require no maintenance, no replacement, and do not lose their optical power over time.
Unlike some other forms of vision correction, there is no regression, which is why refractive lens exchange is often described as a one-time solution. The procedure offers a lasting improvement in vision that can be relied upon for decades.
From a long-term perspective, the results are remarkably stable, providing clear and consistent vision across near, intermediate, and distance tasks. This durability is one of the key benefits that makes RLE an attractive option for presbyopia and high prescriptions.
Emotional readiness matters more than people realise
Undergoing refractive lens exchange is not just a physical decision; it’s also an emotional one. You need to feel comfortable with the idea of eye surgery and understand that the goal is functional vision, not perfection.
Being mentally prepared helps you navigate the process calmly and confidently. Patients who approach the procedure with curiosity and realistic expectations are usually the most satisfied with the results.
Accepting that there may be a short adaptation period or minor visual phenomena, and focusing on the overall improvement, makes the experience far more rewarding.
Why consultation quality is everything
A rushed consultation is a red flag when considering refractive lens exchange (RLE). This highly personalised procedure requires careful measurement, discussion, and planning to achieve the best possible outcome. Taking time ensures that your unique needs and priorities are fully considered.
- Personalised assessment is essential: Successful RLE depends on understanding your lifestyle, work, hobbies, and visual goals. These factors guide lens selection and the surgical approach, ensuring the procedure fits your individual needs.
- Thorough discussion improves outcomes: Patients should feel fully heard, with all questions answered and concerns addressed. A detailed consultation allows the surgeon to tailor the plan for the clearest, most comfortable vision.
- Specialist centres provide focused expertise: Centres that specialise in lens-based vision correction, such as RLE Surgery in London at the London Cataract Centre, combine technical skill with patient-focused care. Their expertise ensures that every aspect of the procedure is carefully planned and executed.
A thorough consultation is critical to the success of refractive lens exchange. Taking the time to personalise the plan improves outcomes and patient satisfaction. Choosing a specialist centre ensures both expertise and a focus on your individual visual needs.
Recovery and adjustment timeline
Most people notice a significant improvement in vision within just a few days after surgery. However, full stabilisation and adaptation take longer, and this is a normal part of the recovery process. Your brain and eyes need time to adjust to the new lens, especially with multifocal or extended-range designs. Some mild fluctuations in vision, glare, or halos may occur initially.
Follow-up care is an essential part of the journey. Experienced providers monitor your progress closely and address any concerns proactively. Regular check-ups help ensure the lens is performing as expected and that adaptation is progressing smoothly. With proper care, most patients achieve stable, comfortable vision within a few weeks.
During this adaptation period, it’s important to follow all post-operative instructions carefully. Avoid strenuous activity, protect your eyes from dust and bright sunlight, and use prescribed eye drops as directed. Being patient and attentive to your recovery helps maximise the benefits of RLE and supports long-term visual comfort.
Common misconceptions about RLE and presbyopia
Many people believe refractive lens exchange is only for cataract patients, but that is no longer true. It is now commonly used to correct presbyopia and high prescriptions before cataracts develop. Awareness of this expands treatment options for those seeking clearer vision.
Some assume RLE is too extreme or risky. In reality, for patients with presbyopia or very high prescriptions, it is often safer and more predictable than pushing laser surgery beyond its limits. Proper assessment and experienced surgeons make the procedure highly reliable.
Understanding what the procedure actually involves helps cut through these myths. Accurate information allows patients to make informed decisions. It also highlights the long-term benefits and stability RLE can provide.
Comparing RLE with ongoing optical correction
Glasses and contact lenses require constant attention and updating. Prescriptions change over time, frames can break, lenses may scratch, and contact lens tolerance can decrease as you age. Managing these ongoing needs can be both inconvenient and costly.
Refractive lens exchange replaces this continual maintenance with a one-time surgical intervention. The artificial lens provides stable, long-term vision without the need for frequent updates.
For many patients, this shift from ongoing management to lasting clarity feels liberating. It reduces daily hassles and offers a sense of freedom from corrective eyewear.
Who is not a good candidate?
Refractive lens exchange (RLE) is highly effective, but it is not suitable for everyone. Certain medical conditions and personal factors can make the procedure risky or less beneficial. Careful evaluation ensures that patients receive the safest and most appropriate treatment.
- Pre-existing eye conditions: Conditions such as severe glaucoma or retinal disease can increase surgical risk or reduce the effectiveness of RLE. Thorough eye assessments are essential to identify these factors before proceeding.
- Expectations and mindset: Unrealistic expectations or significant fear of surgery can make RLE a poor choice. Patients must understand both the benefits and limitations to make an informed decision and avoid disappointment.
- Importance of honest assessment: A responsible surgeon prioritises safety and may recommend alternative treatments if RLE is unsuitable. This ensures the patient’s long-term vision and wellbeing remain the primary focus.
RLE is not a one-size-fits-all solution. Careful evaluation of eye health, expectations, and personal suitability helps ensure safe, successful outcomes. Choosing a surgeon who prioritises honesty and safety protects both vision and overall wellbeing.
The psychological impact of stable near vision

Regaining comfortable near vision can be surprisingly emotional. Many people don’t realise how much mental energy they’ve spent compensating for presbyopia each day. Once that burden lifts, routine tasks like reading, cooking, or using a phone feel much easier.
This newfound clarity can boost confidence and independence. Patients often notice a reduction in daily frustration and eye strain. The sense of visual freedom can improve overall wellbeing.
The psychological benefit of stable near vision is often underestimated but deeply felt. It goes beyond function, positively affecting mood, productivity, and quality of life.
FAQs:
1. What is presbyopia and why does it happen?
Presbyopia is the age-related stiffening of the eye’s natural lens, which reduces the ability to focus on near objects. It usually starts in your early to mid-40s and progresses over time, making reading glasses necessary for close work.
2. Why don’t glasses or contact lenses “fix” presbyopia?
Glasses and contact lenses only compensate for presbyopia. They manage symptoms but do not address the underlying lens stiffening, so reliance on corrective eyewear continues and often increases with age.
3. Can laser eye surgery correct presbyopia permanently?
No. Laser procedures reshape the cornea but leave the natural lens in place, so presbyopia continues to progress. This makes laser surgery a temporary solution rather than a permanent fix for near vision.
4. How does refractive lens exchange (RLE) treat presbyopia?
RLE replaces the eye’s natural lens with an artificial intraocular lens. By removing the ageing lens responsible for presbyopia, it restores near, intermediate, and distance vision depending on the lens type chosen.
5. Are the results of RLE permanent?
Yes. The implanted lens does not age or lose flexibility, so presbyopia caused by lens stiffening does not return. Other eye conditions may still develop, but the presbyopia correction itself is lasting.
6. What types of lenses are used in RLE?
Options include monofocal lenses (sharp vision at one distance), multifocal lenses (vision at multiple ranges), and extended depth-of-focus lenses (smooth intermediate vision). Each type balances clarity, range, and potential visual side effects differently.
7. Will I be completely free from glasses after RLE?
Many patients achieve high levels of spectacle independence, especially with multifocal or extended-range lenses. Some may still need glasses for very fine print or low-light tasks, but everyday vision is usually functional without corrective lenses.
8. What is neural adaptation and why is it important?
After RLE, the brain needs time to adjust to the new lens. Neural adaptation allows the eyes to switch focus between near, intermediate, and distance tasks. Temporary glare, halos, or minor visual fluctuations are normal during this adjustment period.
9. When is the best age to consider RLE for presbyopia?
RLE is typically recommended for patients in their late 40s to early 60s, once near vision has declined and the natural lens has limited flexibility. Younger patients with minimal presbyopia may not benefit as much.
10. What makes a good candidate for RLE?
Ideal candidates have presbyopia or high prescriptions, healthy eyes, and realistic expectations. Certain conditions, such as advanced glaucoma or retinal disease, may make RLE unsuitable, highlighting the need for thorough evaluation by an experienced surgeon.
Final Thoughts: Achieving Long-Term Near Vision Freedom
Refractive lens exchange (RLE) offers a truly permanent solution for presbyopia by replacing the ageing natural lens with a stable artificial intraocular lens. Unlike glasses, contact lenses, or laser procedures, RLE addresses the root cause of near vision decline, providing reliable vision across near, intermediate, and distance ranges. While adaptation and minor visual phenomena can occur initially, most patients experience a lasting improvement that simplifies daily life, reduces eye strain, and enhances overall confidence.
Choosing the right lens type, working with an experienced surgeon, and having a thorough consultation are all critical to achieving the best outcome. By focusing on personalised care and long-term stability, RLE can significantly improve your visual independence and quality of life. If you’re looking for RLE surgery in London, you can get in touch with us at London Cataract Centre.
References:
- Kohnen, T., Refractive lens exchange: Advances, indications and outcomes. Refractive Lens Exchange, https://pubmed.ncbi.nlm.nih.gov/25127929/
- Trojacka, E., 2025. Current trends in presbyopia correction: Overview of surgical and refractive methods including lensbased approaches. Journal of Clinical Medicine, https://www.mdpi.com/2077-0383/15/1/215
- Stern, B., 2025. Presbyopia correction in lens replacement surgery: A review. Clinical & Experimental Ophthalmology. https://pmc.ncbi.nlm.nih.gov/articles/PMC12326228/
- Khoramnia, R. & Naujokaitis, T., 2024. Functional outcomes after refractive lens exchange with multifocal/EDOF intraocular lenses: Spectacle independence and visual performance https://www.sciencedirect.com/science/article/pii/S0002939424003519
- Cochener, B. et al., 2023. Visual outcomes and patient satisfaction after bilateral refractive lens exchange with trifocal intraocular lenses in presbyopic patients. https://pubmed.ncbi.nlm.nih.gov/37052874/