")

One of the most common questions I hear from patients considering lens replacement is: “Will I still need glasses?” It’s completely understandable the main goal for many is to reduce dependence on spectacles. However, the answer isn’t simply yes or no, as it depends on the type of intraocular lens (IOL) chosen, your visual goals, and the anatomy of your eyes.
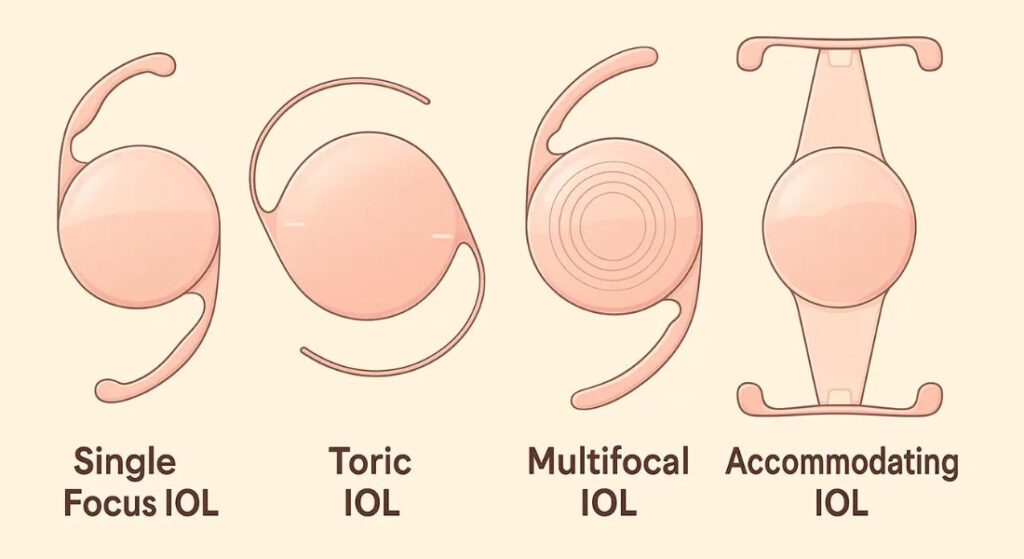
Standard monofocal lenses reliably restore distance vision, but most patients still require reading glasses for near tasks. This is because monofocals are optimised for a single focal point, meaning close-up activities like reading or smartphone use typically remain dependent on spectacles. Understanding this limitation upfront helps manage expectations and ensures satisfaction after surgery.
Premium lenses, such as multifocal, toric, or extended depth-of-focus (EDOF) IOLs, are designed to expand the range of clear vision. Multifocals provide multiple focal points for near, intermediate, and distance vision, while EDOF lenses create a smooth range of focus with minimal night-time visual disturbances. Toric IOLs address astigmatism, further reducing the need for corrective glasses.
I guide each patient through a personalised decision-making process, considering lifestyle, hobbies, and visual priorities. By explaining the benefits and trade-offs of each lens type, patients can choose the option that best balances independence from glasses with visual quality, ultimately achieving functional vision tailored to their daily life.
Standard Monofocal IOLs: Clear Distance Vision
Standard monofocal lenses are the most commonly implanted IOLs worldwide, designed primarily to provide excellent distance vision. They perform reliably for activities like driving, watching TV, or recognising faces across a room, giving patients sharp, consistent far vision.
The main limitation is near and intermediate vision. Reading glasses are usually still needed for tasks like using a phone, working on a computer, or reading a menu. Some patients explore monovision, correcting one eye for distance and the other for near tasks, but this requires brain adaptation and isn’t suitable for everyone.
Despite the trade-off, standard monofocals remain a dependable choice for patients prioritising distance vision. Proper pre-operative counselling ensures patients understand the limitations, helping them enjoy functional vision safely and confidently post-surgery.
Toric IOLs: Distance Vision Plus Astigmatism Correction
Astigmatism can leave patients with blurred or distorted vision even after standard lens implantation. Toric IOLs are designed specifically to address this corneal irregularity while restoring clear distance vision. For patients who prioritise sharpness and clarity, these lenses offer a measurable improvement over monofocals. Understanding the scope of correction distance versus near is critical to aligning expectations.
- Correction of Corneal Irregularities: Toric lenses neutralise the irregular curvature of the cornea, directly reducing distortion and blurred vision. This correction improves overall visual comfort, particularly for distance activities like driving or watching television. The precise alignment of the lens is essential to achieve optimal results.
- Focus on Distance Vision: Standard toric lenses primarily address distance vision, meaning most patients will still require reading glasses for near tasks. The lens eliminates the astigmatic blur but does not extend focus across multiple distances. This distinction helps patients understand the limits and benefits of a toric-only solution.
- Option for Multifocal Toric Lenses: Patients who want both astigmatism correction and reduced near-vision dependence can consider multifocal toric lenses. These combine distance correction with intermediate and near focus, offering broader visual independence. Careful patient selection and counselling are critical to ensure satisfaction with this more complex option.
- Improved Visual Comfort: By eliminating corneal blur and distortion, toric lenses enhance comfort for daily distance activities. Patients experience sharper, more stable vision, reducing eye strain and reliance on corrective lenses. The real-world impact is smoother visual performance and greater confidence in routine tasks.
Toric IOLs are a targeted solution for astigmatic patients seeking crisp distance vision. When properly aligned and paired with realistic expectations, they provide a meaningful reduction in blur and a clear improvement in visual comfort. Proper assessment and lens choice remain the keys to achieving predictable, high-quality outcomes.
Multifocal IOLs: Reducing Dependence on Glasses

Multifocal IOLs are engineered to split incoming light into multiple focal points, providing clear vision at distance, intermediate, and near. Many patients with these lenses achieve significant freedom from glasses, often handling reading, computer work, and driving without corrective eyewear.
Adaptation is an important part of the process. Initially, some patients notice halos, glare, or mild blur in certain lighting conditions. Over time, the brain adjusts to processing the multiple focal points, and these visual phenomena generally become less noticeable.
These lenses are particularly well suited to patients who prioritise independence from spectacles across all distances. Careful assessment of lifestyle needs and visual expectations ensures that multifocal IOLs deliver functional vision while minimising early adaptation challenges.
Extended Depth-of-Focus (EDOF) Lenses: Smooth Vision Transition
EDOF lenses represent a newer class of premium IOLs, engineered to provide a continuous range of vision while minimising the optical side effects often seen with traditional multifocals. They perform particularly well for distance and intermediate vision, and generally offer functional near vision for most everyday tasks.
I often recommend EDOF lenses for patients seeking a balance: minimal glare or halos, smooth transitions between distances, and reduced reliance on reading glasses. While spectacles may still be needed for very fine print, the overall dependence is significantly lower than with standard monofocals.
These lenses are ideal for patients with active lifestyles or work that requires frequent switching between different visual distances. Proper pre-operative assessment ensures the lens choice aligns with both anatomical factors and functional vision goals, maximising satisfaction and daily convenience.
Realistic Expectations for Near, Intermediate, and Distance Vision
Patients often assume one lens type will give perfect vision at all distances, but each IOL has inherent strengths and limits. Being upfront about what each lens can realistically achieve prevents disappointment and enhances satisfaction. The goal is to match lens choice with the patient’s lifestyle and visual priorities, not to promise complete spectacle independence for everyone. Clear explanations help patients make informed decisions that align with their daily needs.
- Distance Vision: Almost all IOL types monofocal, toric, multifocal, and EDOF deliver reliable distance vision. Patients rarely need glasses for driving, outdoor activities, or watching TV. This consistency makes distance vision the most predictable outcome across lens types.
- Intermediate Vision: Standard monofocals usually require glasses for tasks like computer work or reading a car dashboard. Multifocal and EDOF lenses improve functional intermediate vision, reducing dependency on spectacles for these activities. Choosing the right lens for intermediate tasks can dramatically enhance day-to-day convenience.
- Near Vision: Monofocal lenses almost always require reading glasses for close tasks. Multifocal lenses often reduce or eliminate this need, while EDOF lenses provide functional near vision for most tasks but may struggle with very fine print. Patients should understand that some compromise may still exist depending on the lens type and individual anatomy.
- Setting Realistic Expectations: “Freedom from glasses” is achievable, but the degree varies with lens choice, corneal anatomy, and daily visual demands. Transparent counselling helps patients appreciate the benefits without overpromising. This alignment between expectation and reality is essential to satisfaction and long-term confidence in the outcome.
Managing expectations carefully ensures patients enjoy the visual independence premium lenses can provide. By clarifying what is realistic at each distance, we prevent surprises and reinforce trust in both the lens choice and the surgical process. Ultimately, informed patients are happier patients.
Factors Influencing Post-Operative Glasses Use
Several factors determine whether patients will still need glasses after IOL surgery. The type of lens chosen monofocal, toric, multifocal, or EDOF has the most direct impact on post-operative dependence. Pre-existing eye conditions, such as macular changes or corneal irregularities, can influence how well the lens performs for both distance and near tasks, affecting the overall need for spectacles.
Dominant eye selection and monovision strategies can reduce reliance on reading glasses, but these approaches require adaptation and aren’t suitable for every patient. Lifestyle and visual priorities play a major role: those who read frequently, work extensively on digital devices, or need precise near vision may still require glasses for certain tasks.
Other practical considerations include age, pupil size, and ocular surface health, all of which can subtly affect visual outcomes. By assessing these factors thoroughly, I help each patient select a lens that aligns with both their anatomical needs and day-to-day activities. This personalised approach maximises independence from spectacles while setting realistic, achievable expectations for post-operative vision.
Adaptation and Neuro-Visual Learning
For multifocal and EDOF lenses, adaptation is a critical phase in achieving optimal functional vision. The brain must learn to process the multiple focal points created by these lenses, and during this period, some patients notice halos, glare, or slight blur, particularly in low-light conditions or at night. Early awareness of these phenomena helps set realistic expectations and reduces post-operative anxiety.
I reassure patients that most of these visual side effects diminish within weeks as the brain adapts. Encouraging adherence to post-operative instructions, including gentle visual exercises and gradual resumption of near tasks, supports faster neuro-visual learning and smoother transition to independent vision.
Follow-up appointments are essential during this adaptation period. They allow me to monitor progress, adjust any minor issues, and provide guidance tailored to the patient’s lifestyle and visual goals. With structured support, the majority of patients achieve stable, functional vision and enjoy a significant reduction in reliance on glasses for everyday activities.
Combining IOL Choices for Best Outcomes
Not every patient achieves optimal vision with a single lens type, so I often consider a tailored mix-and-match strategy. The idea is to leverage the strengths of different lenses across each eye to cover the full range of vision. Done correctly, this approach can minimise side effects like halos or glare while enhancing overall visual independence. It requires careful preoperative planning and clear discussion with the patient about expected outcomes.
- Dominant Eye with Multifocal Lens: Placing a multifocal lens in the dominant eye prioritises sharp distance vision while still offering functional near and intermediate focus. This ensures that tasks like driving or watching TV remain effortless. It also forms the anchor for the overall binocular visual system, stabilising perception.
- Non-Dominant Eye with EDOF or Monofocal Lens: The non-dominant eye can receive an EDOF or monofocal lens to support intermediate and near vision. This combination balances the range of focus, reducing reliance on reading glasses for daily activities. The complementary optics between the two eyes help smooth transitions and minimise visual disturbances.
- Reduction of Visual Side Effects: By not using multifocal lenses in both eyes, the likelihood of halos, glare, or contrast sensitivity issues is lowered. Patients experience a more comfortable and natural visual experience, especially in low-light conditions. Careful lens selection and alignment are critical to achieve this balance.
- Patient-Specific Tailoring: Success depends on considering each patient’s visual habits, ocular anatomy, and tolerance for trade-offs. Preoperative simulation and discussion help set realistic expectations. When executed thoughtfully, this personalised strategy maximises spectacle independence without compromising comfort or clarity.
Mix-and-match IOL strategies allow us to harness the benefits of multiple lens technologies while mitigating their limitations. With careful planning and patient-specific adjustments, we can deliver sharper, more versatile vision across all distances.
Post-Operative Considerations
Even after a successful IOL procedure, glasses may still be required for specific tasks. These typically include reading very small print, performing precision work such as sewing or fine crafts, or night driving if minor halos or glare persist. Discussing these possibilities beforehand helps patients form realistic expectations and reduces post-operative anxiety.
For the majority, overall reliance on spectacles decreases dramatically. Daily activities from computer work to driving and casual reading are often achievable without glasses, offering a level of independence that many patients find life-changing. The degree of spectacle freedom depends on lens type, pre-existing eye conditions, and individual adaptation.
I emphasise that post-operative adaptation, diligent follow-up, and adherence to care instructions are as important as selecting the right lens. Regular reviews allow early detection of any visual concerns, guidance on neuro-visual learning, and reassurance that minor optical phenomena are typically temporary. With structured support, patients achieve optimal functional vision and enjoy sustained comfort and independence across a wide range of everyday activities.
Common Misconceptions
Patients frequently assume that premium lenses will completely eliminate the need for glasses. I clarify that no lens can restore perfect vision for every task without some compromise, and individual outcomes vary based on eye anatomy and lifestyle needs.
Monofocal lenses, while highly effective for distance vision, do not address near tasks, whereas premium lenses like multifocal, toric, or EDOF designs reduce dependence on spectacles but may require a period of adaptation. Minor optical phenomena such as halos or glare can occur initially and usually improve as the brain adjusts.
Managing expectations upfront is crucial. Clear discussion about what each lens can realistically achieve ensures patients approach surgery with confidence, understand potential trade-offs, and are satisfied with their post-operative outcomes.
Benefits of Reduced Dependence on Glasses
Even partial freedom from spectacles offers meaningful advantages. Convenience is a major factor patients no longer need to switch between reading and distance glasses multiple times a day, streamlining daily routines.
Safety is another benefit, particularly for night driving or outdoor activities, where clear, uninterrupted vision reduces risk and increases confidence. Lifestyle enhancement also plays a significant role: patients enjoy sports, hobbies, and social interactions without the limitations of glasses.
When lens selection is carefully matched to anatomy, visual needs, and lifestyle, patients consistently report high satisfaction. Minimising dependence on spectacles not only improves functional vision but also contributes to overall quality of life and long-term contentment with their surgical outcome.
Technology and Planning in Modern IOL Surgery
Modern lens replacement relies on meticulous pre-operative assessment to achieve the best possible outcomes. Corneal topography and astigmatism mapping identify subtle irregularities that could affect lens performance, while pupil size and ocular surface evaluation help predict visual quality under varying lighting conditions.
Biometric measurements are critical for selecting the optimal lens type, power, and alignment. These data guide decisions on multifocal, toric, or EDOF lenses, ensuring they match the patient’s anatomy and visual requirements.
This personalised, technology-driven approach minimises the likelihood of needing spectacles after surgery. By combining precise diagnostics with careful planning, I can tailor lens selection to each patient, optimising functional vision and overall satisfaction.
Patient Communication and Shared Decision-Making
I always emphasise that lens choice is a collaborative process. We discuss lifestyle, visual priorities, and the patient’s willingness to adapt to multifocal or EDOF optics. Simulation tools and trial lenses help patients visualise potential outcomes, setting realistic expectations and enhancing satisfaction.
Case examples highlight how personalised lens selection shapes post-operative dependence on glasses: one patient in their 60s with mild astigmatism chose a toric multifocal IOL and achieved excellent distance and near vision, only occasionally needing reading glasses for very fine print. Another patient with high visual demands for computer work opted for an EDOF lens, enjoying minimal reliance on spectacles for intermediate and distance tasks while occasionally requiring them for small text.
These examples demonstrate that glasses use after IOL surgery is highly individualised. It depends on lens type, ocular anatomy, lifestyle, and how the patient adapts to their new visual system, reinforcing the importance of shared decision-making and tailored planning.
Long-Term Outcomes
Long-term studies consistently confirm the performance of different IOL types. Monofocal lenses reliably restore distance vision, but patients almost always require spectacles for near tasks. Multifocal and EDOF lenses, by contrast, provide high rates of independence from glasses, especially for distance and intermediate activities.
Success depends on more than the lens itself. Proper patient selection, thorough pre-operative planning, and guidance during post-operative adaptation are key predictors of functional outcomes and patient satisfaction.
In my clinical experience, these findings are mirrored in everyday practice. Glasses dependence after IOL surgery is largely determined by lens choice, ocular anatomy, and the patient’s lifestyle needs, highlighting the importance of personalised planning and shared decision-making.
Integrating IOL Surgery in London Practices
Selecting an experienced surgeon is crucial for achieving optimal post-operative outcomes. Precision in pre-operative assessment, including corneal mapping, biometric measurements, and lens alignment planning, directly influences functional vision and glasses independence.
Careful lens selection and personalised surgical planning minimise the likelihood of needing spectacles, particularly for multifocal, toric, or EDOF lenses. Patients benefit from a tailored approach that accounts for anatomy, lifestyle, and visual priorities, ensuring both comfort and satisfaction.
For those exploring options, IOL Surgery in London provides comprehensive evaluation and expert guidance. By combining advanced diagnostics with personalised planning, patients gain a clear pathway to achieving functional, high-quality vision with reduced reliance on corrective lenses.
FAQs:
1. Will I still need glasses after IOL surgery?
It depends on the type of IOL. Monofocal lenses usually require reading glasses for near tasks, while multifocal, toric, or EDOF lenses can significantly reduce spectacle dependence.
2. Which IOLs correct astigmatism?
Toric lenses are designed specifically to correct corneal astigmatism, improving distance vision and reducing blur. Multifocal toric lenses can also address near and intermediate vision.
3. Can I achieve complete independence from glasses?
Complete independence isn’t guaranteed. Multifocal and EDOF lenses provide high functional freedom, but reading very small print may still require glasses.
4. How long does it take to adapt to multifocal or EDOF lenses?
Adaptation usually takes a few weeks as the brain learns to process multiple focal points. Mild halos or glare often reduce over time.
5. Are there side effects with premium IOLs?
Some patients notice halos, glare, or slight blur initially. These effects usually diminish with adaptation, particularly with EDOF lenses.
6. Can one eye have a different IOL than the other?
Yes. A mix-and-match approach such as multifocal in the dominant eye and EDOF in the non-dominant eye can optimise vision across all distances and reduce side effects.
7. Do younger patients benefit more from premium IOLs?
Active patients or those with broad visual demands often gain the most, as premium lenses provide functional vision for multiple distances and reduce reliance on glasses.
8. How does pre-existing eye health affect IOL outcomes?
Conditions like macular changes, corneal irregularities, or dry eye can influence visual performance and spectacle dependence. Thorough pre-operative assessment is essential.
9. Will I need glasses for night driving?
Most patients experience clear distance vision at night, though mild halos or glare may occur initially. Adaptation and proper lens selection minimise this risk.
10. How do I choose the right lens for my lifestyle?
Lens selection should align with your daily activities, hobbies, and visual priorities. A personalised consultation, biometric measurements, and trial simulations help determine the best option.
Final Thoughts: Making Glasses Independence Realistic
Glasses use after IOL surgery isn’t a one-size-fits-all outcome it depends on lens type, eye anatomy, lifestyle, and how your brain adapts to new optics. Monofocals reliably restore distance vision but reading glasses are usually still needed, whereas multifocal, toric, and EDOF lenses can dramatically reduce dependence on spectacles across multiple distances. The key to satisfaction lies in careful pre-operative assessment, realistic expectation-setting, and personalised lens selection.
Adaptation is part of the process for multifocal and EDOF lenses, with mild halos or glare often appearing initially. With structured follow-up and guidance, most patients find their brain adjusts within weeks, resulting in functional vision for driving, screen work, hobbies, and everyday tasks without frequent glasses use. Shared decision-making ensures patients choose the lens that aligns with both visual needs and lifestyle demands.
If you’re thinking about IOL surgery in London, you can get in touch with us at London Cataract Centre. A personalised consultation that combines advanced diagnostics with tailored lens planning ensures you enjoy functional, high-quality vision with minimal reliance on glasses.
References:
- Ferguson, T., et al. (2022) ‘Premium intraocular lenses in patients with ocular comorbidities: outcomes and spectacle independence’, Bioengineering, https://www.mdpi.com/2306-5354/10/9/993
- Liu, Y.C., et al. (2022) ‘Visual acuity outcomes and spectacle independence after implantation of multifocal IOLs’, Journal of Ophthalmology, https://pmc.ncbi.nlm.nih.gov/articles/PMC5747227/
- Zvorničanin, J. and Zvorničanin, E. (2018) ‘Premium intraocular lenses: the past, present and future’, Journal of Current Ophthalmology https://www.sciencedirect.com/science/article/pii/S2452232517302561
- Abd-Ellatif, M.A.-E. (2024) ‘Comparison between Intraocular Lenses TECNIS Eyhance™ IOL and AcrySof, QJM: An International Journal of Medicine, Oxford Academic https://academic.oup.com/qjmed/article/117/Supplement_2/hcae175.631/7904120
- Bianchi, G.R. (2020) Spectacle independence after cataract surgery: a prospective study with a multifocal intraocular lens, Medical Hypothesis, Discovery & Innovation in Ophthalmology, https://pmc.ncbi.nlm.nih.gov/articles/PMC6969558/